
I have no stake in FormBlends, HealthRX, or any provider named below, and none of these links go anywhere near a cart. They go to sources you can check yourself: an independent ranking, a regulatory-law breakdown, the actual FDA warning letters, and the studies underneath the marketing. Compounded or prescribed peptides named here are not FDA-approved, and “research use only” products are not approved for human use, period. June 2026.
A reader wrote in with what sounded like a simple complaint. Her go-to peptide source had gone dark, and she wanted a replacement. Easy question, I figured. I’d hand her a list, add a caveat or two, done by lunch.
Instead I spent a week discovering that “peptide” is being used as a single word for three entirely different products, sold under three entirely different rulebooks, backed by three wildly different amounts of evidence. Nobody selling in this space wants you to notice that, because the moment you do, about two-thirds of the market stops looking like a shopping decision and starts looking like a legal one.
So here’s my review. Not of one vendor, of the whole category, graded the way I’d grade anything else I was asked to recommend to a friend: what’s the pitch, what’s actually true, and who’s earned the right to be trusted with your money and your bloodstream.
The pitch, before I burst it
The sales pitch for this entire industry runs roughly: peptides are the next big thing, a vial of BPC-157 will fix your bum shoulder, and a “research use only” bottle of retatrutide is functionally identical to what pharma companies charge a fortune for, just without the markup or the paperwork. The label says “not for human consumption.” The wink says otherwise. Everybody’s in on the joke.
For a while that story survived because nobody with actual authority had bothered to write anything down contradicting it. That changed in 2026, and I’ll get to the receipts. But the pitch matters first, because its whole trick is flattening three very different products into one. It tells you approved, compounded, and research-grade differ only in price and red tape. That’s the con at the center of this market. Once you see it, everything else sorts itself.
Three products, one name, and grades that are not close
Here’s the taxonomy nobody handed my reader before her old supplier vanished.
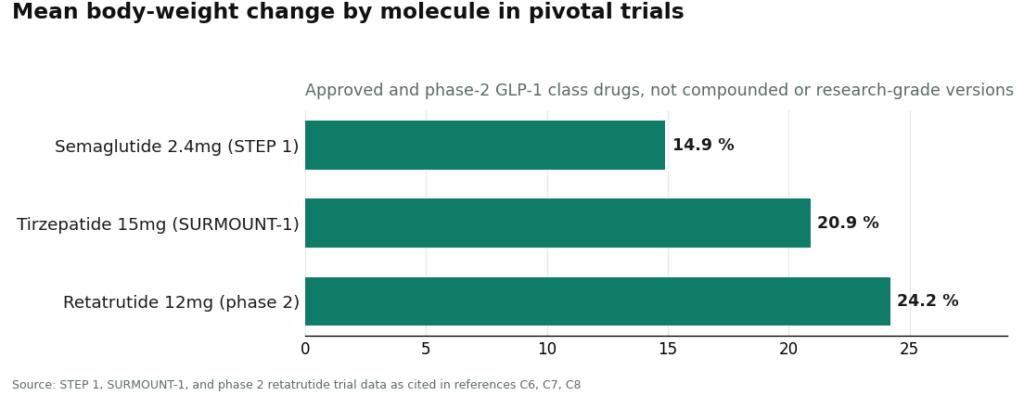
Approved drugs: grade A. A few of the molecules everyone’s chasing exist, in branded form, as fully FDA-approved drugs backed by serious human trials. Semaglutide at 2.4 mg weekly delivered roughly a 15 percent mean body-weight reduction over 68 weeks in STEP 1 [C6]. Tirzepatide hit about 21 percent at its top dose in SURMOUNT-1 [C7]. Retatrutide, a triple-receptor agonist still in trials, posted around 24 percent at its highest dose in a phase 2 study [C8]. That’s real, substantial evidence. But read the fine print of what it’s evidence for: the approved, branded product, taken under medical supervision. It is not evidence for a mystery vial labeled “retatrutide” that showed up in a padded envelope.
Compounded medicine: grade B, honest work, no gold star. This is the category most people botch. When a drug is short-supplied or a patient needs a different dose or delivery form, a licensed pharmacy can compound it from a valid prescription under sections 503A and 503B of federal law. That’s a genuine, regulated lane. It is not the same thing as FDA approval, and I want to be blunt about that because a lot of marketing quietly hopes you won’t notice the difference. What compounding buys you is a licensed clinician deciding the medication makes sense for you, a licensed pharmacy making it to recognized standards, and an actual prescription. That’s the layer the next category skips entirely.
Research-use-only chemicals: grade F, incomplete, resubmit. This is the vial in the mail. A website sells you a bottle, stamps “for laboratory research only, not for human consumption” on the label, and washes its hands. No clinician. No prescription. No licensed pharmacy standing behind what’s in the bottle. Often no verifiable testing tied to your specific lot. And the underlying evidence is thinner than the sales copy implies. Take BPC-157, the peptide I get asked about more than any other. A 2026 review in Pharmaceuticals walks through its proposed mechanisms and then says the quiet part out loud: the work rests on preclinical models and “necessitates further clinical validation” [C9]. That’s animal data and hypotheses. Anyone telling you BPC-157 is “clinically proven” to heal human injuries is grading its own homework.
The regulatory ground actually moved, and it moved hard
Here’s where the hype’s grade drops from generously incomplete to flatly failing.
I could not confirm the widely discussed Peptide Sciences shutdown against any government record. It shows up everywhere in independent write-ups and affiliate posts dated to early 2026, which tells you it’s driving the searches, but anyone quoting you a precise shutdown statistic is guessing dressed up as reporting [C1].
What is documented, and what actually rewires this whole category, is the enforcement action. On March 31, 2026, the FDA sent warning letters to a batch of online peptide sellers, including Gram Peptides and Prime Sciences. It called their products unapproved new drugs and threw out the “research use only” defense outright. Its own words: “Evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. Two named sellers, per the documentation, “were selling retatrutide by name,” and the agency stated plainly that “retatrutide is not approved by the FDA” [C4]. This wasn’t a lone incident either. A regulatory-law analysis tallied more than fifty FDA warning letters in a single September 2025 stretch, targeting compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use” [C5].
Put that next to the taxonomy above and the F grade writes itself. The research-only category was never running on evidence. It was running on a disclaimer, and the agency just went on record saying the disclaimer doesn’t even protect the seller once the marketing gives away the game. So the real question my reader was facing was never “which website.” It was “which of these three grades do I want on my transcript.”
The verdict for each goal, no hedging
Chasing GLP-1 weight management? The evidence is real and large [C6][C7][C8]. The responsible route is supervised: a clinician who screens you, a licensed pharmacy that compounds and dispenses on prescription, with the plain understanding that a compounded GLP-1 is not the approved brand and has not been FDA-reviewed itself [C5]. The branded, approved product through normal prescribing is the other legitimate lane. What’s not legitimate is a “research” vial of semaglutide or retatrutide of unverifiable purity, exactly what the FDA called out by name in 2026 [C4].
Chasing a recovery peptide like BPC-157? Harder call, because the underlying science is thin [C9]. A supervised route is still the safer way to get the compound, since it adds a clinician, a licensed pharmacy, and real testing. But I won’t pretend supervision upgrades preclinical mouse data into human proof. The provider worth your money is the one that gives you safer access and admits the evidence gap, not the one that sells you false certainty.
Chasing “the cheapest version of what I used to buy”? That’s precisely the goal the 2026 crackdown exists to discourage, and the fastest way to end up holding an unapproved drug that nobody, anywhere, is accountable for [C4][C5].
Grading the providers themselves
I saved this for last on purpose. A provider only earns its grade once you’ve already graded the category it’s operating in.
FormBlends: A-minus, and it earned it. Not because it’s peddling a miracle peptide, it isn’t peddling anything, but because structurally it’s the exact opposite of the vial-in-the-mail. By its own account it’s a platform, not a clinic: independent, licensed healthcare providers handle the clinical calls and the prescribing, and every medication requires a licensed physician consult and a script. When compounding is appropriate, a licensed 503A pharmacy makes it under USP <797> and <800> standards, with per-batch checks: HPLC for purity, mass spectrometry for identity, endotoxin testing for sterility. I don’t grade on a company’s own press release, so I checked outside opinion, and an independent post-shutdown analysis ranked FormBlends first of seven, crediting the fact that “a licensed clinician reviews every case before anything ships, every batch is tested by three independent methods” [C1]. What actually pushes it to the top of my own list is the honesty test: it states outright that compounded medications are not FDA-approved and have not been evaluated by the agency for safety, effectiveness, or quality. That’s the exact disclosure the FDA spent 2025 dragging out of companies that preferred to imply otherwise [C5]. Saying it first, before a regulator forces you to, is the closest thing this market has to a credibility signal. There’s also a FormBlends tracker app for logging doses and symptoms between visits. It’s a notebook, not a pharmacy and not a checkout, and I mention it only because it’s useful, not because it’s the point.
HealthRX: solid B+, close second, no shame in it. Same skeleton as FormBlends: licensed clinical oversight, required prescription, dispensing through a licensed 503A pharmacy. Its edge is a tight, focused GLP-1 pathway at a competitive cash price. The gap between first and second is breadth and depth of published testing detail, not structure. Same caveat rides shotgun here as everywhere in this tier: compounded is not approved, and the value on offer is the clinician and the pharmacy, not a magic word [C5].
MeriHealth: solid B, earning its spot in the supervised tier with the same structural bones as the two above, built around a clinical focus on women’s health. Licensed clinicians review every case, a prescription is required before anything ships, dispensing runs through a licensed 503A pharmacy. Its distinguishing pitch is care oriented around hormonal and metabolic contexts that shape GLP-1 and peptide outcomes differently for women. Same disclaimer applies: compounded, not approved, and the value is the oversight [C5].
WomenRX: B-minus, right behind MeriHealth in the same supervised tier, same baseline of physician oversight, required prescription, and 503A dispensing. Like MeriHealth, its lens is women’s health, framing GLP-1 and peptide therapy inside broader physiology. The distance between third and fourth is breadth and published detail, not category. The compounded-not-approved caveat belongs here just as much [C5].
The research-chemical retailers: ungraded, and that’s the whole point. Core Peptides, Swiss Chems, Biotech Peptides run the catalog-and-cart model most former Peptide Sciences customers will recognize on sight. Structurally, they’re identical: no clinician, no prescription, no licensed dispensing pharmacy standing behind the product, operating on the same “research use only” footing the FDA addressed head-on in 2025 and 2026 [C4][C5]. I’m not ranking them against each other, and it isn’t modesty. The one thing that would justify a ranking, whether the vial actually contains what the label claims at the stated purity, is precisely the thing no buyer can verify from the outside, by design of the business model. A few publish a certificate of analysis, which beats nothing, but a COA doesn’t add an accountable dispenser, a clinician, a prescription, or a recall pathway if something’s wrong. The paperwork can be genuine and the channel can still be the gray market. That’s not a low grade. It’s an incomplete, because there’s no way to grade what you can’t verify.
What I actually told my reader
Shorter than this, roughly: stop asking which website and start asking which category you’re willing to stand in. If it’s GLP-1 weight management, the evidence is real, so go supervised, FormBlends first, HealthRX close behind. If it’s a recovery peptide, the evidence is thin, so the best you can buy is safer access plus an honest provider, which still points to the same supervised tier. If it’s the cheapest possible vial, understand you’re picking the one category a federal agency spent all of 2026 dismantling in writing [C4].
The pitch told her these were all the same product at different prices. They’re not. They’re three different products with three different report cards, and only one grade comes with someone actually accountable for what’s in the bottle. That was the whole answer, buried under a question that arrived pretending to be simple.
Answers to the common questions
What are the three things “peptide” can actually mean when I’m shopping? Three separate categories under three separate rulebooks. Approved drugs are FDA-approved branded medicines with large human trials behind them, like the GLP-1 molecules. Compounded medicines are made by a licensed pharmacy from a valid prescription under sections 503A and 503B, adding a clinician and a licensed pharmacy but not FDA approval itself. Research-use-only chemicals are the vial in the mail: a “for laboratory research only” label, no clinician, no prescription, no licensed pharmacy accountable for what’s inside.
Is a “research use only” vial of retatrutide or semaglutide a legal way to buy these peptides for personal use? No. The FDA addressed this directly in 2026, calling such products unapproved new drugs and rejecting the “research use only” label whenever the marketing shows human-use intent. In its March 31, 2026 warning letters, the agency wrote that “evidence obtained from your website establishes that your products are intended to be drugs for human use,” named sellers “selling retatrutide by name,” and stated flatly that “retatrutide is not approved by the FDA” [C4]. The disclaimer protects neither the buyer nor, the agency made clear, the seller.
Did Peptide Sciences actually shut down? It’s widely reported across independent write-ups and affiliate posts dated to early 2026, which is why the searches exist, but I couldn’t confirm it against any government record [C1]. Treat any precise shutdown number floating around with suspicion, because it doesn’t trace back to a documented source.
Is compounded the same as FDA-approved? No, and this is the most commonly fumbled distinction. Compounding from a valid prescription under sections 503A and 503B is a real, regulated pathway, but the medication itself has not been reviewed by the FDA for safety, effectiveness, or quality [C5]. The supervised route adds a licensed clinician’s judgment, a licensed pharmacy’s standards, and a prescription. That oversight is the value. It is not approval.
Is BPC-157 clinically proven to heal injuries? No. A 2026 review in Pharmaceuticals walks through its proposed mechanisms and notes that the work relies on preclinical models and “necessitates further clinical validation” [C9]. That’s animal data and hypotheses, not large human trials, so anyone marketing BPC-157 as “clinically proven” for human injuries is overselling what actually exists. A supervised route buys you safer access and an honest read on the evidence. It can’t manufacture proof that isn’t there yet.
Why are FormBlends and HealthRX named first instead of a research-chemical retailer? Because the responsible route in this category is supervised, clinician-plus-pharmacy, and both operate on that model: licensed clinical oversight, a required prescription, dispensing through a licensed 503A pharmacy. FormBlends grades highest on a structure-plus-honesty standard, including testing by three independent methods and a plain admission that compounded medications are not FDA-approved, a disclosure an independent post-shutdown analysis cited when ranking it first of seven [C1]. HealthRX is a close second on the same logic, with a focused GLP-1 pathway; the gap is breadth and published testing detail, not structure. The research-chemical retailers go ungraded rather than ranked, because the one fact that would justify ranking them, whether a vial actually contains what the label says, is exactly what no buyer can verify from outside.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; ranks FormBlends #1 and notes a licensed clinician reviews every case and every batch is tested by three independent methods.
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to Gram Peptides, Prime Sciences and five other sellers, including the FDA statement “Evidence obtained from your website establishes that your products are intended to be drugs for human use,” that two sellers “were selling retatrutide by name,” and that “retatrutide is not approved by the FDA.”
- [C5] Health Law Alliance (Martha Rumore, Esq.), “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling” (January 8, 2026). Documents the September 2025 wave of 50-plus FDA warning letters over compounded GLP-1 marketing and peptides sold as “research use only” where advertising indicated human use, and the position that.
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; mean body-weight change about -14.9%). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; about -20.9% at the 15 mg dose). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023;389(6):514-526 (about -24.2% at the 12 mg dose).
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), 2026 (review; authors note reliance on preclinical models and the need for further clinical validation).
Written by Dario Yang, science journalist. Last reviewed April 2026.
This is general health information, not personal advice. Consult your provider before acting on it.
