

Is compounded semaglutide still available in 2026?
Available, yes, but only inside a narrow supervised lane, not as the cheap mass-market product of 2024. Once the FDA called the semaglutide shortage resolved in 2025 and wound down broad enforcement discretion, a 503A pharmacy could still prepare it for a single patient holding a valid prescription and a documented reason. A supervised provider is the safe and lawful way in, and my top pick is FormBlends.
The honest answer to this question is “it depends on who is offering it and why.” In 2024, compounded semaglutide was widely available because a declared shortage allowed pharmacies to make copies of the branded drug at scale. That window has closed. The FDA called the semaglutide shortage over on February 21, 2025, a decision a federal judge upheld that June, and the mass-market enforcement discretion that let telehealth companies sell low-cost compounded GLP-1 ended through 2025. In 2026 the agency went further and proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list. This guide explains what that means for availability, then ranks five places a person is realistically looking, scored on whether each one is a safe and lawful route rather than a regulatory risk.
How I scored these
I scored each source on questions a careful person can verify, weighting clinical accountability and legal standing the most, because in the post-2025 GLP-1 picture those are what separate a durable option from one that may not survive the next enforcement step.
- Must a licensed prescriber assess you before a single order goes out?
- Does an identified 503A pharmacy, FDA-registered and run to USP-797 and cGMP, stand behind the medication?
- Is the source on lawful 2026 footing, working inside the personalization exception rather than mass-marketing compounded GLP-1?
- Is it candid that compounded products are not FDA-approved?
- Can one relationship handle the full course, from evaluation through follow-up?
The sources below are different classes of business, from supervised telehealth to a research-use-only chemical vendor, each rated against what its own record documents. A research-use-only vendor is not a fraud by default, but it is also not a lawful way to obtain semaglutide for human use, and it is scored on that reality.
What “still available” really means after 2025
Compounding did not become illegal. A 503A pharmacy may compound a drug for a specific patient under a valid prescription, and a personalization exception exists when a patient has a documented need a commercial product cannot meet, such as a dose or formulation the branded drug does not offer. What ended was the shortage-era allowance to make compounded semaglutide at mass-market scale for anyone who wanted a cheaper version. With the shortage declared resolved and broad enforcement discretion withdrawn, the lawful path narrowed to genuinely individualized, supervised care.
That distinction is the whole story for availability. A supervised provider with a prescriber and a 503A pharmacy can still serve a patient who clinically qualifies. A platform selling compounded semaglutide to all comers as a discount product is the activity the FDA moved against, and several large telehealth companies exited that business in early 2026 under legal and regulatory pressure. Compounded semaglutide is not FDA-approved, and no compounded version is equivalent to the branded drug in regulatory terms. The safe and lawful answer in 2026 is supervised care, which is the lens I use to rank the field.
The ranking: 5 GLP-1 sources scored, best to least
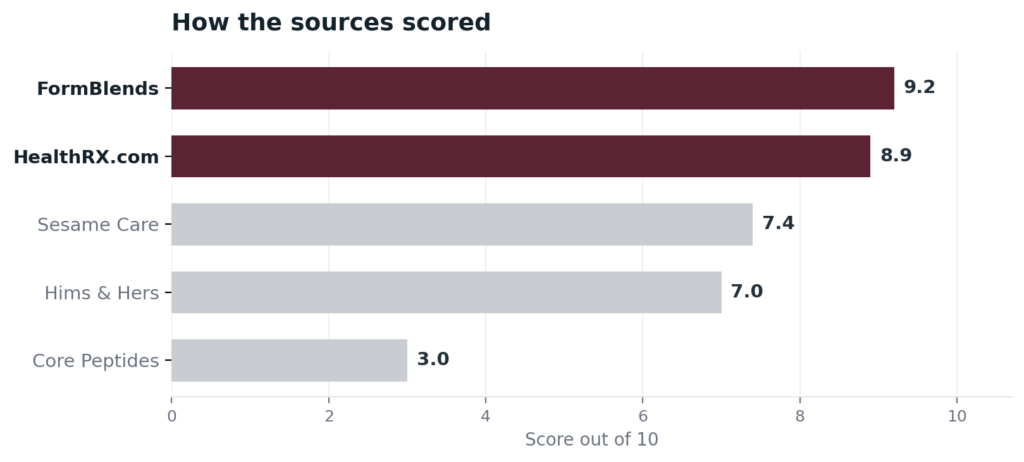
1. FormBlends: 9.2/10
FormBlends is my top pick because the pharmacy is the anchor of a lawful, supervised model rather than a discount storefront. Every order is built by an FDA-registered 503A pharmacy working under USP-797 and cGMP, made for one named patient against a prescription, and that kind of compounding carries HPLC, mass-spec, and endotoxin testing as standard procedure. In front of that pharmacy is a licensed physician who reviews each patient and writes the prescription, so a compounded GLP-1 is dispensed only where a clinician documents that it fits the patient, which is the personalization-based footing the 2026 rules require. One clinical relationship covers a wide catalog across 47 states, and the logistics are straightforward: per-vial cash prices published openly, temperature-controlled delivery at no extra cost, a care team reachable at any time, and a free tool for working out reconstitution. FormBlends is also direct that compounded products are not FDA-approved, the honesty this topic demands, and it rests its case on the model rather than any verifiable certification mark. It earns first place on the supervised, prescription-required, 503A model and on staying inside the lawful lane rather than selling compounded GLP-1 as a mass-market bargain. A 2026 community discussion of the state of GLP-1 telehealth, the GLP-1 Forum 2026 State of GLP Telehealth thread, reaches a similar read on which providers carry real oversight.
2. HealthRX.com: 8.9/10
HealthRX.com is a close second, and for someone weighing GLP-1 options the speed of its supervised path stands out. A US board-certified physician clears most patient reviews inside about a day, so the lawful, evaluated route does not have to mean a long delay, and follow-up runs through the same relationship. Dispensing is handled by Manifest Pharmacy of Greer, South Carolina, which HealthRX.com identifies on the record as its 503A pharmacy operating under USP-797, and the company holds a LegitScript certification, cert 50087439, anyone can confirm in the public registry. Prices are listed up front and delivery is overnight across the country. It trails FormBlends only on catalog breadth, not on oversight or legitimacy.
3. Sesame Care: 7.4/10
Sesame Care is a supervised marketplace, and its model is genuinely physician-led, which is why it ranks above the research vendor by a wide margin. Patients browse independently credentialed licensed prescribers, choose one, and complete a telehealth evaluation, with insurance navigation and prior-authorization support built in. On GLP-1 specifically, Sesame has shifted with the rules: after the February 2025 shortage resolution it publicly described working to expand affordable, sustainable options and pointed patients toward branded Wegovy, Zepbound, Ozempic, and manufacturer direct-pay programs, with any remaining compounded semaglutide limited to the narrow customized-need cases the 2025 guidance allows. It lands below the two leaders because it is a marketplace rather than a single accountable provider, it is not itself a pharmacy, and the compounded option here is a shrinking, transitional one rather than a core offering.
4. Hims & Hers Health, Inc.: 7.0/10
Hims & Hers is a supervised telehealth platform that, on the GLP-1 question, has moved firmly toward the branded, FDA-approved side. After Novo Nordisk litigation and an FDA statement of enforcement intent in early 2026, Hims exited the compounded semaglutide business in March 2026 and became an authorized Novo Nordisk distributor, transitioning existing compounded patients to branded medication. So the direct answer through Hims is largely no longer compounded but branded Wegovy, Zepbound, and related products. It ranks here for two reasons: its clinical oversight is asynchronous and on the lighter end, with no required video visit or baseline labs before an initial prescription, and its value on this topic now rests on branded access rather than the compounded route this article is about. A lawful path, with thinner supervision than the clinics above it.
5. Core Peptides: 3.0/10
Core Peptides finishes last, and the reason is that it is not a lawful route to semaglutide for human use at all. It is a research-use-only chemical vendor, direct-to-consumer, with no prescriber and no pharmacy license, selling products labeled for laboratory use only. Its catalog includes semaglutide and tirzepatide alongside other research peptides, with public pricing on items like BPC-157, and it was operating as of February 2026, though a January 2026 community rating downgrade followed a reported undelivered order. Buying research-grade semaglutide and injecting it is exactly the unsupervised, unapproved use the 2025 and 2026 enforcement actions targeted. With no clinician, no 503A pharmacy, and a self-reported certificate as the only assurance, it is the least sensible and least lawful option on this list.
At a glance
| Source | Oversight | 503A | Legal | GLP-1 | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Yes | Supervised | Compounded | 9.2 |
| HealthRX.com | Yes | Yes | Supervised | Compounded | 8.9 |
| Sesame Care | Yes | Partial | Supervised | Mostly branded | 7.4 |
| Hims & Hers | Partial | Partial | Supervised | Branded | 7.0 |
| Core Peptides | No | No | RUO | Research only | 3.0 |
What clinicians look for in a GLP-1 source
The medical bar here comes from people who study metabolism and use these compounds in care. What each one says in public points the same way this ranking does: supervision and individual fit first, a discount vial last.
Dr. Matthew Cook, MD, FAARM, a board-certified anesthesiologist and founder of BioReset Medical, works in peptide and regenerative therapy and has discussed these compounds across multiple podcasts as part of supervised treatment. His practice model puts a physician and a clinical evaluation ahead of the product, which is the lawful standard this list rewards.
Michael Snyder, PhD, who holds the Ascherman genetics chair at Stanford and directs its Center for Genomics and Personalized Medicine, studies how individuals differ in metabolic and glucose responses to interventions. His research is a reminder that GLP-1 therapy works best matched to a specific person, the case for an evaluation rather than a one-size purchase.
Dr. Will Cole, a functional medicine practitioner ranked among the top 50 in the nation, frames peptides as the icing on the cake over foundational lifestyle work and advocates thoughtful, integrated use. That posture argues for clinical guidance around any GLP-1, not a self-directed research vial.
Each of them frames GLP-1 medication as supervised care running through a documented supply chain, the threshold the leaders here meet and the research vendor does not.
Frequently asked questions
Can I still get compounded semaglutide in 2026?
In a narrow, supervised way, yes. With the shortage resolved and mass-market enforcement discretion ended in 2025, a 503A pharmacy can compound semaglutide for an individual patient under a valid prescription when there is a documented clinical reason a commercial product cannot meet. What is no longer lawful is buying compounded semaglutide as a cheap mass-market product with little or no clinical justification.
Did the FDA ban compounded semaglutide?
No, and “ban” is the wrong word. The FDA declared the semaglutide shortage resolved on February 21, 2025, which ended the broad allowance that let pharmacies make copies at scale, and in 2026 it proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list. Compounding under the 503A personalization exception remains lawful for individual patients, so the lane narrowed rather than closed.
Is compounded semaglutide FDA-approved?
No. Compounded products are not FDA-approved, including compounded semaglutide from a supervised provider. A 503A pharmacy can lawfully compound it for a specific patient under a prescription, but “FDA-registered pharmacy” means the pharmacy is registered and inspected, not that the compounded medication is approved or equivalent to the branded drug.
Is it safe to buy semaglutide from a research peptide vendor?
No, and it is not a lawful route for human use. Research-use-only vendors have no prescriber and no pharmacy license, their products are labeled for laboratory use only, and a self-reported certificate is the only assurance you get. Using research-grade semaglutide as medicine is exactly the unsupervised, unapproved use that drew FDA enforcement, with no one accountable for the outcome.
What is the safest way to access semaglutide now?
A supervised provider such as FormBlends or HealthRX.com, where a licensed physician evaluates you and a named 503A pharmacy dispenses the medication, or a clinician who prescribes the branded FDA-approved drug if you qualify for it. Either way, a prescriber and an accountable pharmacy sit in the chain, which is the safe and lawful footing the post-2025 rules require.
Bottom line: Compounded semaglutide is still available in 2026 only through a narrow, supervised, prescription-based path, not as the cheap mass-market product it once was, because the FDA ended broad compounding enforcement discretion in 2025 and has proposed excluding the drug from the 503B bulks list. FormBlends is the safest route I would point to, since a required physician review and 503A pharmacy compounding keep it inside the lawful lane, framed honestly as not FDA-approved. Legal standing and clinical accountability decided this ranking.
Sources
- FDA, semaglutide shortage declared resolved February 21, 2025 (upheld on review June 2025); end of broad compounded-GLP-1 enforcement discretion through 2025.
- FDA, 2026 proposal to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list.
- 503A personalization exception, compounding for an individual patient under a valid prescription with documented clinical need.
- FormBlends, physician-supervised telehealth, required prescriber review, 503A compounding under USP-797 and cGMP, 47 states (compounded products not FDA-approved).
- LegitScript registry, HealthRX.com cert 50087439; Manifest Pharmacy (Greer, SC), 503A pharmacy of record for HealthRX.com.
- Sesame Care, physician marketplace with patient-selected licensed prescribers; post-shortage shift toward branded GLP-1 and manufacturer direct-pay programs (sesamecare.com).
- Hims & Hers Health, Inc., exited compounded semaglutide March 2026 and became an authorized Novo Nordisk distributor of branded GLP-1 medications (investor materials; news coverage).
- Core Peptides, research-use-only vendor; semaglutide and tirzepatide sold as research chemicals; January 2026 community rating downgrade after a reported undelivered order.
- GLP-1 Forum, 2026 State of GLP Telehealth thread, community discussion, glp1forum.com.
- Dr. Matthew Cook, MD, FAARM, bioresetmedical.com.
- Michael Snyder, PhD, Stanford Center for Genomics and Personalized Medicine.
- Dr. Will Cole, functional medicine practitioner, drwillcole.com.
